What Is Tip Projection & How Do You Improve It? — Part I
Tip projection is a term that surgeons use all the time, but that still confuses many patients and surgeons.
Some of this confusion is inevitable because so many surgeons perform open rhinoplasty. If the skin is not connected to the nose and under its usual tension, it is simply impossible to understand or assess tip projection.
Tip projection is a reflection of how strong the tip cartilages are. The tip cartilages must project the lower nasal skin out far enough to create a straight bridge. Without adequate tip projection, you cannot have a straight profile.
The reference point that I use to assess projection is the end of the bridge just above the tip (see the blue arrows on the left and middle photos). If the tip itself reaches to that point, that’s adequate projection. If the tip sticks way out beyond the bridge, that’s excessive projection. [Shown in the photo on the left]. If the tip hangs off the end of the bridge, that’s inadequate projection because the bridge is holding the tip up [Shown in the photo in the middle] – – the tip can’t support itself independently.
The key anatomical structure that determines whether tip projection is adequate is the central segment of the tip cartilages, the so-called middle crus. (See the drawing on the right with the circle). If that segment is long enough, the tip projects adequately.
Tip projection reflects tip cartilage strength, not lower nasal size. This is an important distinction. The photos in this slide show two patients who have lower noses of different size, but the smaller nose (on the left) has excessive projection and the larger nose (in the middle) has inadequate projection. Skin volume and cartilage strength are two different things. This is an important distinction for the surgeon to make before setting and operative plan.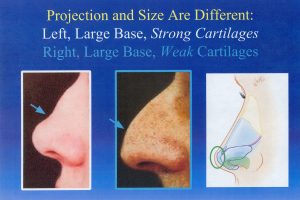
This is the end of Part I.
See you next week.